|
Calculating Total Body Surface Area (TBSA) is crucial in determining initial fluid resuscitation and potential disposition. The Rule of 9s is inaccurate and consistently overestimates TBSA by about 20% which can lead to over-resuscitation. For TBSA <15%: The Rule of Palms is highly accurate and easy to teach. Use the size of the patient's hand (including the fingers) to estimate burn size. https://emergencymedicinecases.com/burn-inhalation-injuries/ 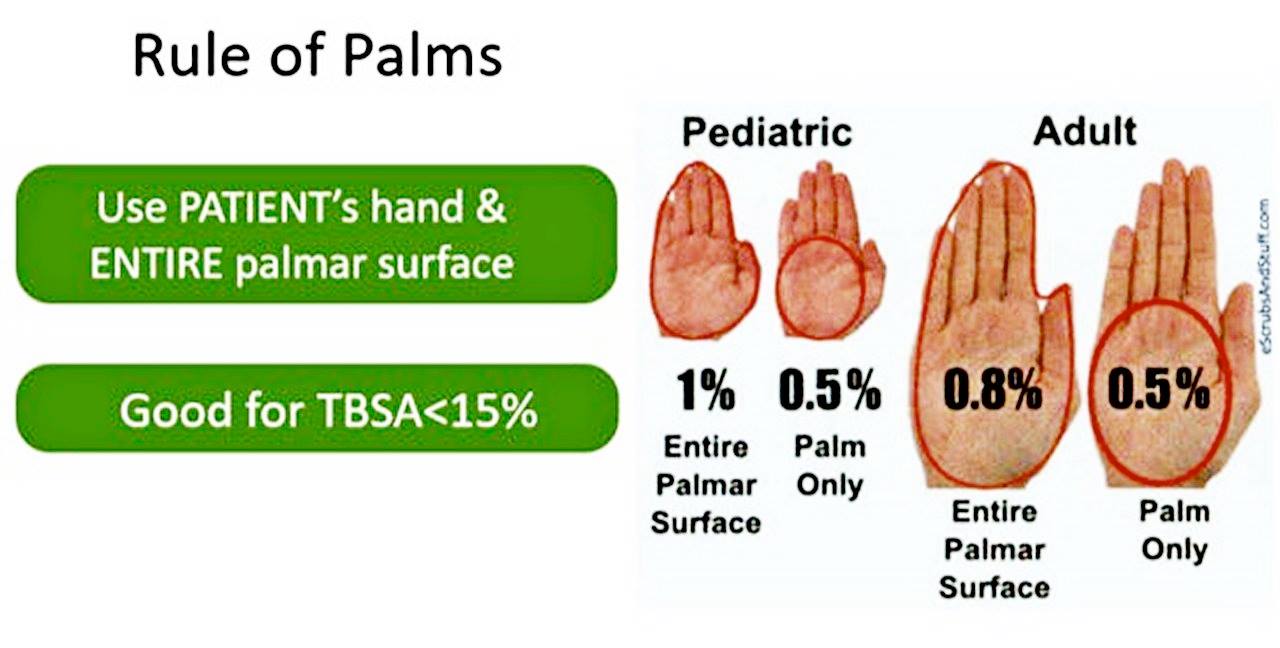 Lemierre’s syndrome - septic thrombophlebitis of the internal jugular vein Lemierre’s syndrome is an uncommon complication of pharyngitis usually caused by Fusobacterium necrophorum, an anaerobe, that leads to suppurative thrombophlebitis of the internal jugular vein and subsequent disseminated infection, often with septic pulmonary emboli. It usually presents as a prolonged pharyngitis in a patient who is febrile, appears ill, has asymmetric anterior neck swelling, often pleuritic chest pain, shortness of breath, and often tachypnea with abnormal oxygen saturation. It is diagnosed with CT neck (and usually chest) with contrast. It’s treated with broad spectrum antibiotics that cover anaerobes, such as piperacillin-tazobactam or ampicillin-sulbactam, often in an ICU setting. https://westjem.com/diagnostic-acumen/lemierres-syndrome.html https://www.nejm.org/doi/pdf/10.1056/NEJMicm1808378 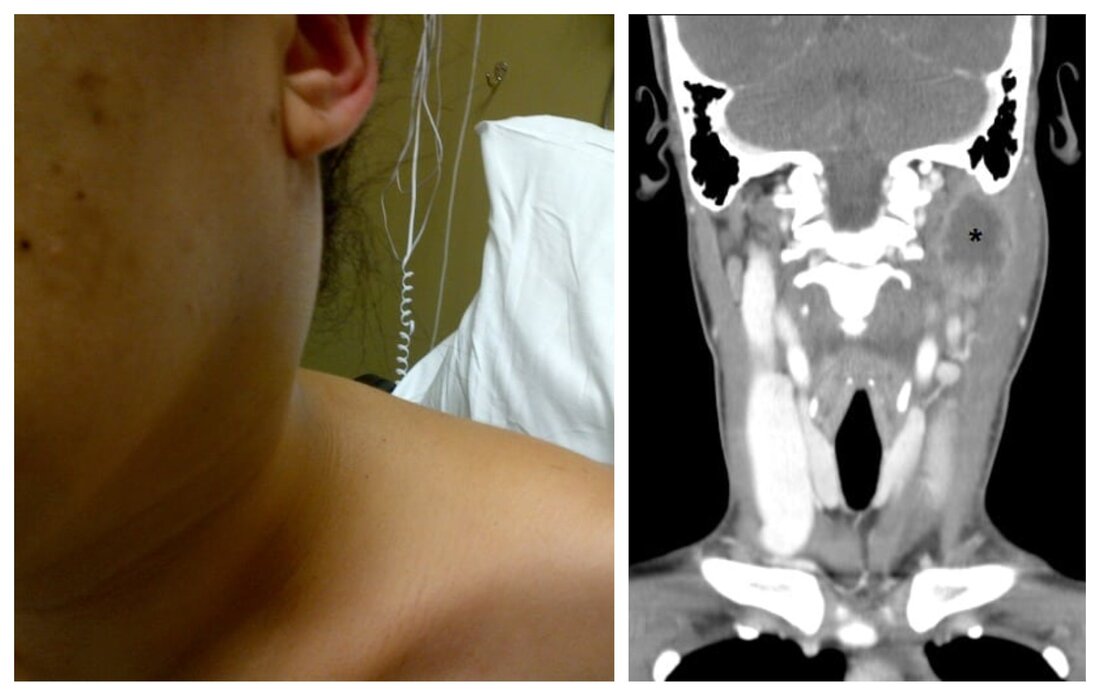 Modified Brooke/Parkland Formula The formula is recommended as a starting point for fluid resuscitation for burns >15% BSA in children and >20% BSA in adults. Titrate rate of fluid for a urine output of 30-50cc/hr in adults and 0.5-1cc/kg/hr in children. Increase or decrease resuscitation fluid rate by 30% if hourly target not reached. https://emergencymedicinecases.com/burn-inhalation-injuries/ 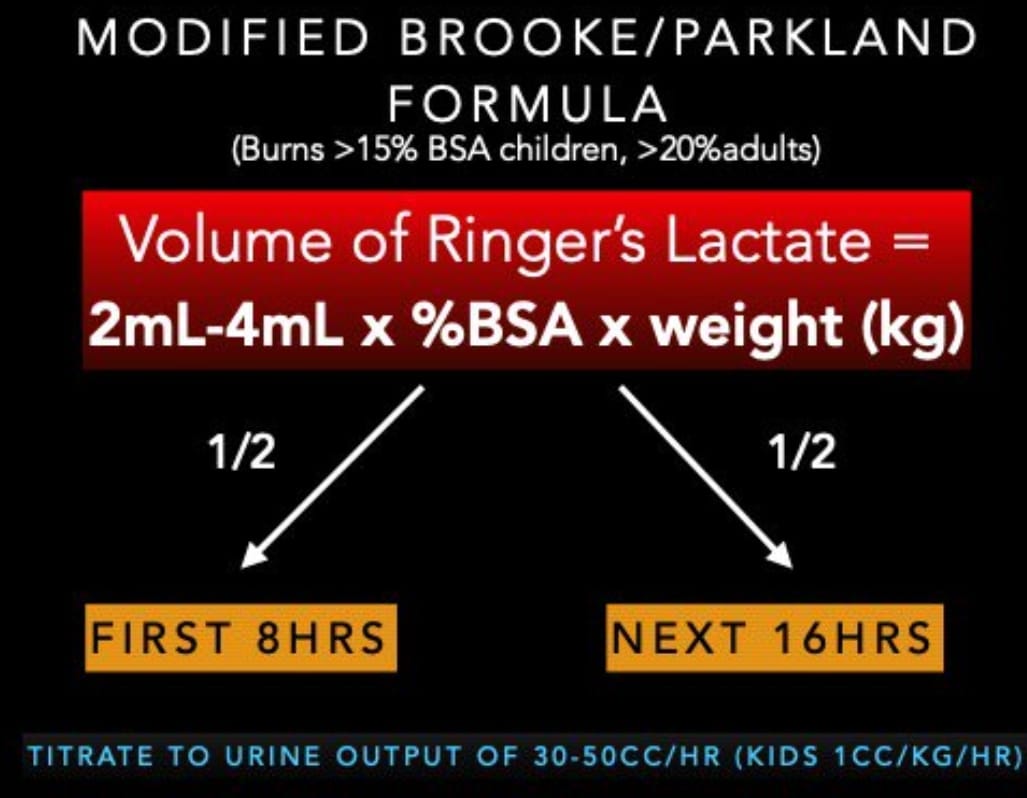 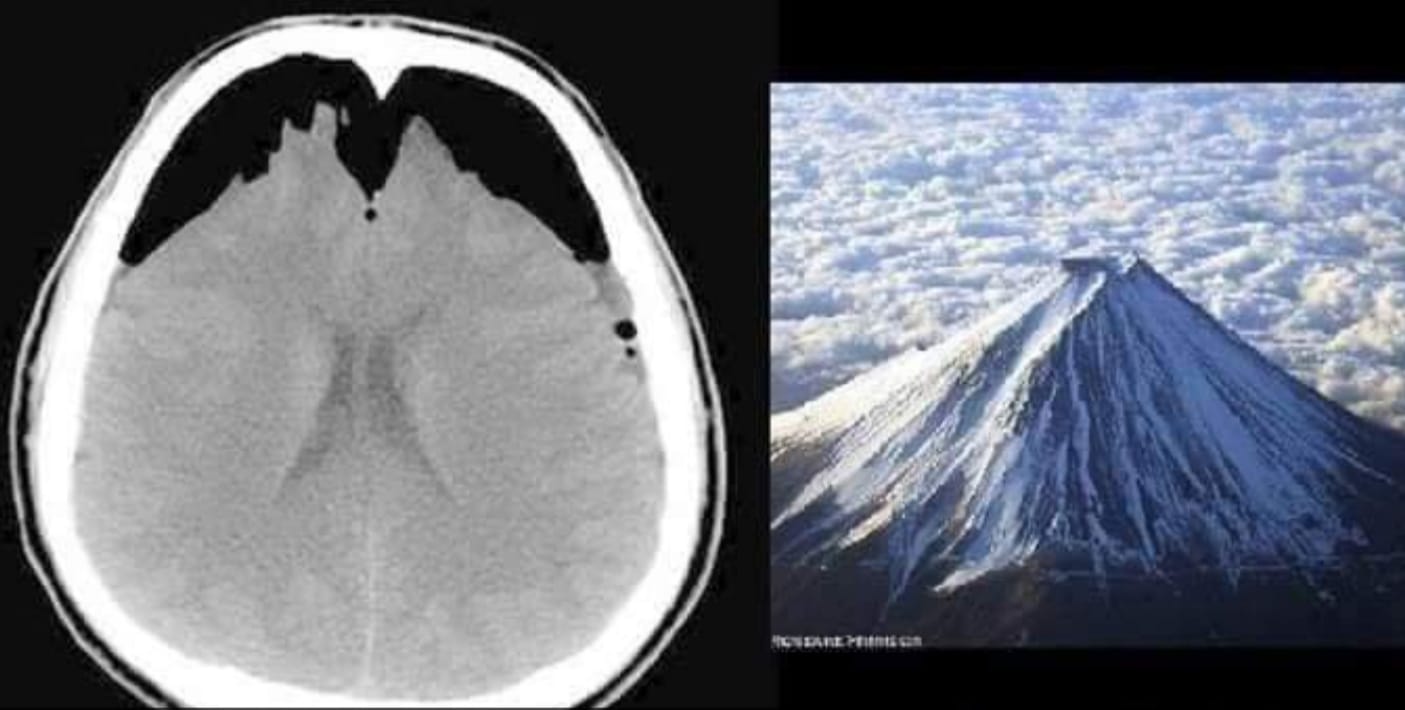 The mount Fuji sign of tension pneumocephalus
Tension pneumocephalus is a neurosurgical emergency that occurs when subdural air causes a mass-effect over the underlying brain parenchyma, often from a ball-valve mechanism causing one-way entry of air into the subdural space . https://radiopaedia.org/articles/tension-pneumocephalus Reverse triage for lightning-strike MCI Reverse triage is essential in lightning-strike induced mass casualty incident (MCI) since those who appear dead may be easily resuscitated with good survival rates, so should be attended to first. Patients sufferring from lightning strike may initially have fixed and dilated pupils (autonomic dysfunction) and cold mottled extremities from vasospasm. Asystole occurs from direct depolarization of the myocardium but typically spontaneous ROSC is achieved. Respiratory arrest from medullary paralysis can take longer to resolve and patients may develop a secondary hypoxic arrest. https://emergencymedicinecases.com/electrical-injuries/ 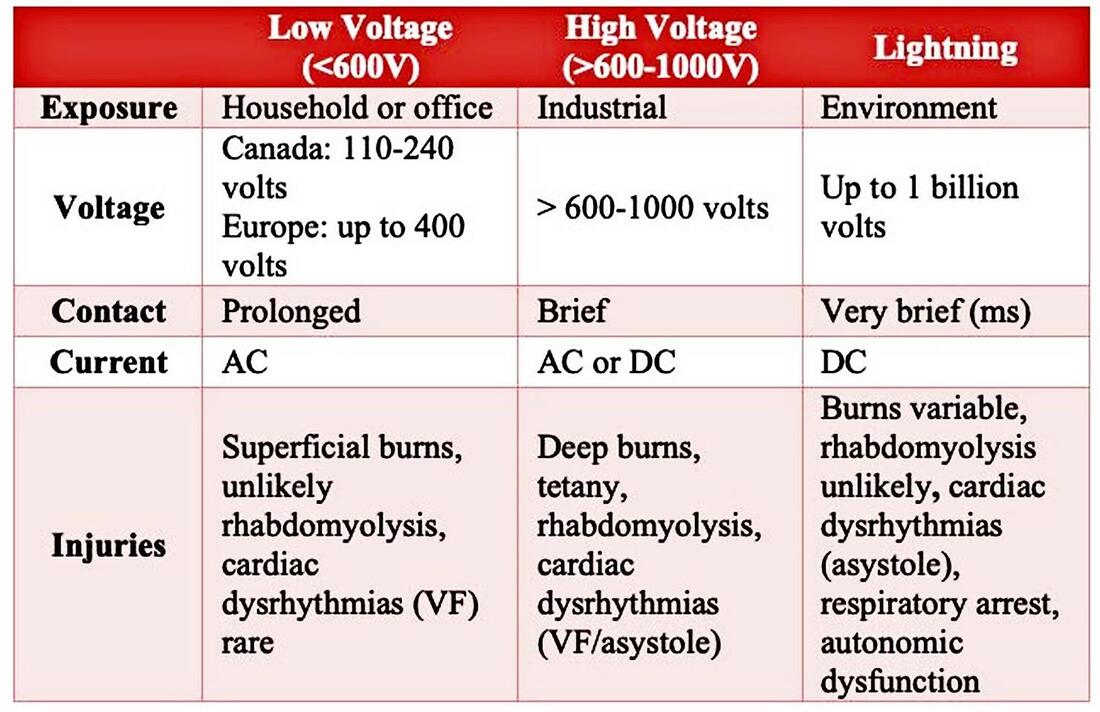 |

Author
|