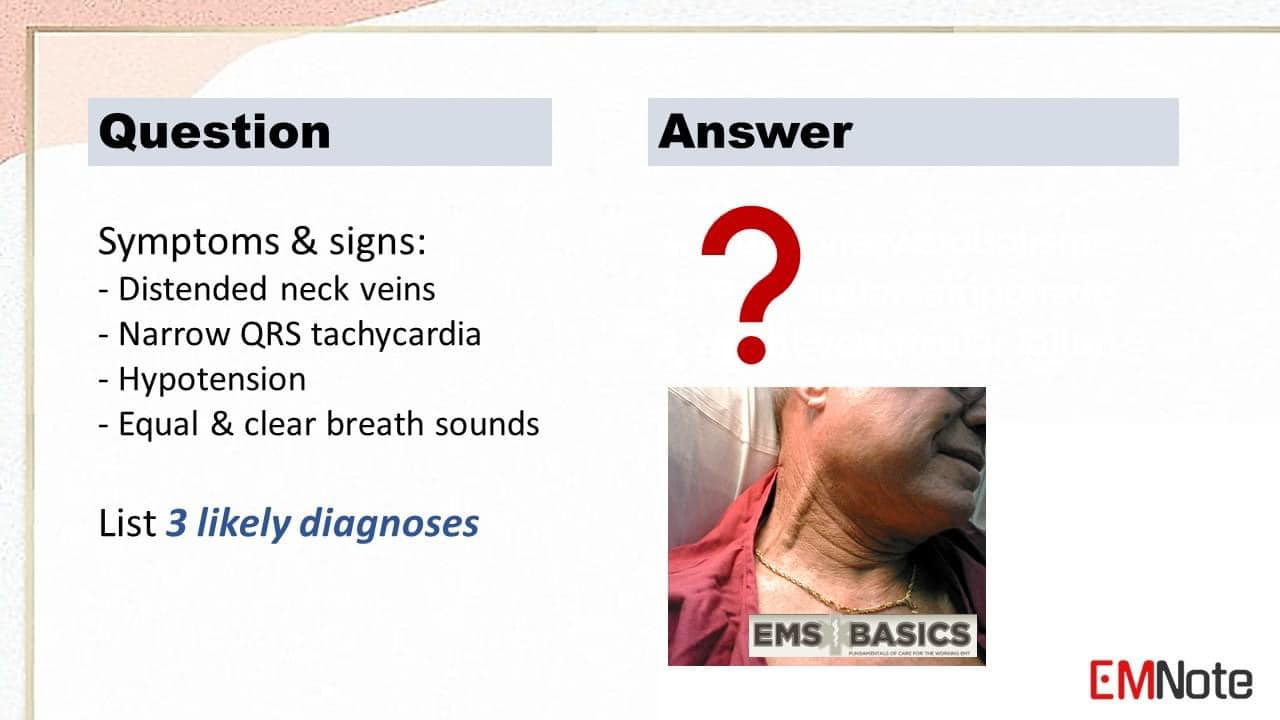
 Treatment of HYPERKALEMIA
1. Calcium gluconate ■ 10 cc 10% IV over 10 min. 2. Insulin with glucose ■ 10 U insulin + 50 cc D50W IV push. 3. Salbutamol nebulizer ■ 10 mg in 4 cc NS nebulized over 10 min. 4. Sodium bicarbonate ■ 1-2 mEq/Kg IV push. 5. Furosemide ■ 40 mg IV. 6. Polystyrene sulfonates ■ Kayexalate or Kalimate. 7. Hemodialysis ■ If all above treatments fail or patient with renal failure.  Visual Diagnosis Part 9
Isolated ulnar shaft fracture is also known as “nightstick fracture.” The injury occurred during an assault, where the patient raised his arm in self-defense. Healthcare provider should consider the possibility of elder abuse or intimate partner violence. Anterior wall myocardial infarction due to proximal LAD total occlusion. The De Winter T wave pattern represents a form of ST-segment elevation myocardial infarction (STEMI) involving the left anterior descending (LAD) artery, characterized by ST-segment depression with an upsloping morphology in the precordial leads, often accompanied by tall and peaked T waves. It is associated with a significant risk of complete occlusion of the artery and subsequent myocardial infarction if left untreated. Gouty arthritis usually involves the first metatarsophallengeal joint. The following medications can precipitate gout: Furosemide, Aspirin, Cyclosporine, Thiazide diuretics, Salicylates, Pyrazinamide, Levodopa, Alcohol, Chlorthalidone, and Ethambutol. High lateral wall STEMI with South African flag sign. The ECG Features of High Lateral Wall STEMI consist of ST elevation primarily localized to leads 1, aVL and V2, and reciprocal ST depression in inferior leads, most pronounced in lead 3. The South Africa Flag sign refers to ST elevation in leads 1, aVL and V2, with reciprocal changes best seen in leads 3 and aVF. Aortic dissection involving the ascending aorta. The intimal flap of the ascending aorta can be demonstrated by ultrasound in the suprasternal notch view using a cardiac probe. Acute epiglottitis The thumb sign is a rounded thickening of the epiglottic shadow on a lateral neck x-ray, giving it the appearance of an adult sized thumb. Digital HSV infection is also known as herpetic whitlow. Children with primary HSV-1 gingiva-stomatitis may develop herpetic whitlow associated with thumb and finger sucking. Addison's disease Addison's disease, also known as primary adrenal insufficiency, is a rare condition where the adrenal glands don't produce enough of the essential hormones cortisol and aldosterone. The most common etiology of Addison's disease is autoimmune destruction. Symptoms of Addison's disease include: Chronic fatigue, weakness, weight loss, muscle cramps, nausea and vomiting, hyperpigmentation, and low blood pressure. Diagnosis of Addison's disease include: Blood tests to measure cortisol and aldosterone levels, and ACTH stimulation test. Treatment of Addison's disease include: Lifelong hormone replacement therapy with cortisol and fludrocortisone, and management of underlying cause.  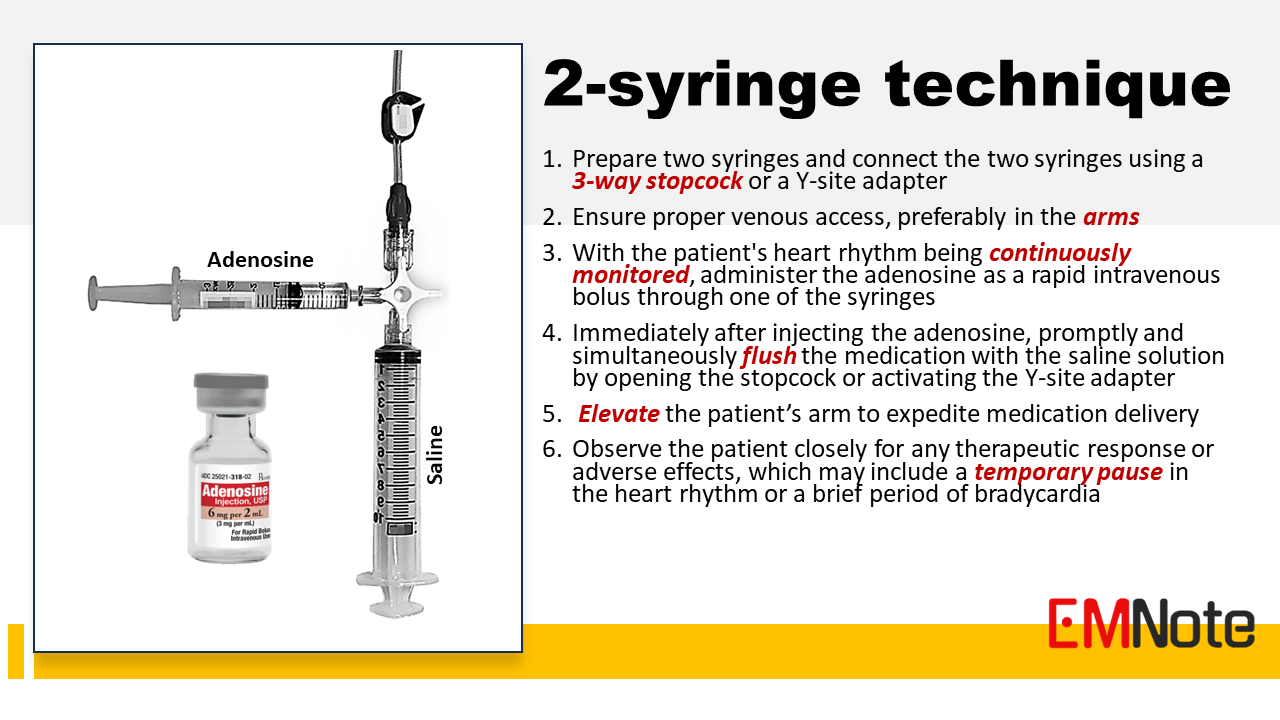 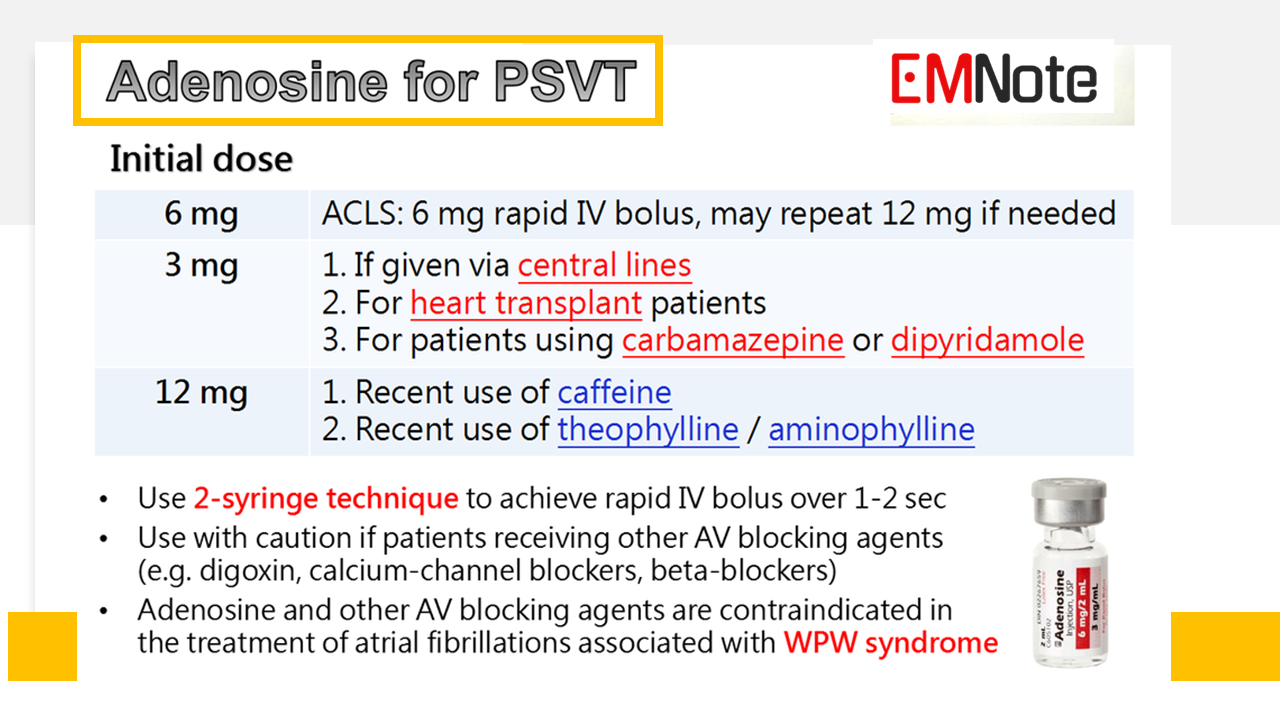 Adenosine for PSVT (ACLS)
- Adenosine is commonly used for the treatment of Paroxysmal Supraventricular Tachycardia (PSVT). - It acts by blocking the AV node and interrupting the re-entry circuit responsible for tachycardia, restoring normal sinus rhythm. - The initial recommended dose is 6 mg, given as a rapid intravenous bolus, followed by a flush of normal saline. - If the first dose doesn't terminate the tachycardia, a second dose of 12 mg may be administered. - Adenosine has a short half-life and may cause a brief period of asystole or bradycardia immediately after administration. The 2-syringe technique The 2-syringe technique allows for the adenosine to be delivered rapidly and efficiently, optimizing its effectiveness in terminating PSVT. It ensures that the medication is promptly delivered to the patient's systemic circulation, enhancing its ability to reach the cardiac tissue and interrupt the re-entry circuit responsible for the tachycardia. 1. Prepare two syringes: One syringe contains the adenosine medication while the other syringe is filled with a saline flush solution. Connect the two syringes using a three-way stopcock or a Y-site adapter. This allows for simultaneous administration of the adenosine and the saline flush solution. 2. Ensure proper venous access: A large-bore intravenous line is typically used to facilitate the rapid delivery of the medication, preferably in the upper extremities. 3. With the patient's heart rhythm being continuously monitored, administer the adenosine as a rapid intravenous bolus through one of the syringes. 4. Immediately after injecting the adenosine, promptly and simultaneously flush the medication with the saline solution by opening the stopcock or activating the Y-site adapter. This helps ensure that the adenosine reaches the systemic circulation quickly. 5. Elevate the patient’s arm to expedite medication delivery 6. Observe the patient closely for any therapeutic response or adverse effects, which may include a temporary pause in the heart rhythm or a brief period of bradycardia. Adenosine dosage - The recommended initial dose of adenosine varies based on specific patient circumstances. Central lines administration, heart transplant patients, or patients using carbamazepine or dipyridamole: The initial dose should be reduced to 3 mg. In patients who have recently consumed caffeine, theophylline, or aminophylline: The initial dose can be increased to 12 mg. - It is contraindicated in patients with second or third-degree heart block, sinus node dysfunction, and patients with atrial fibrillation associated with WPW syndrome.  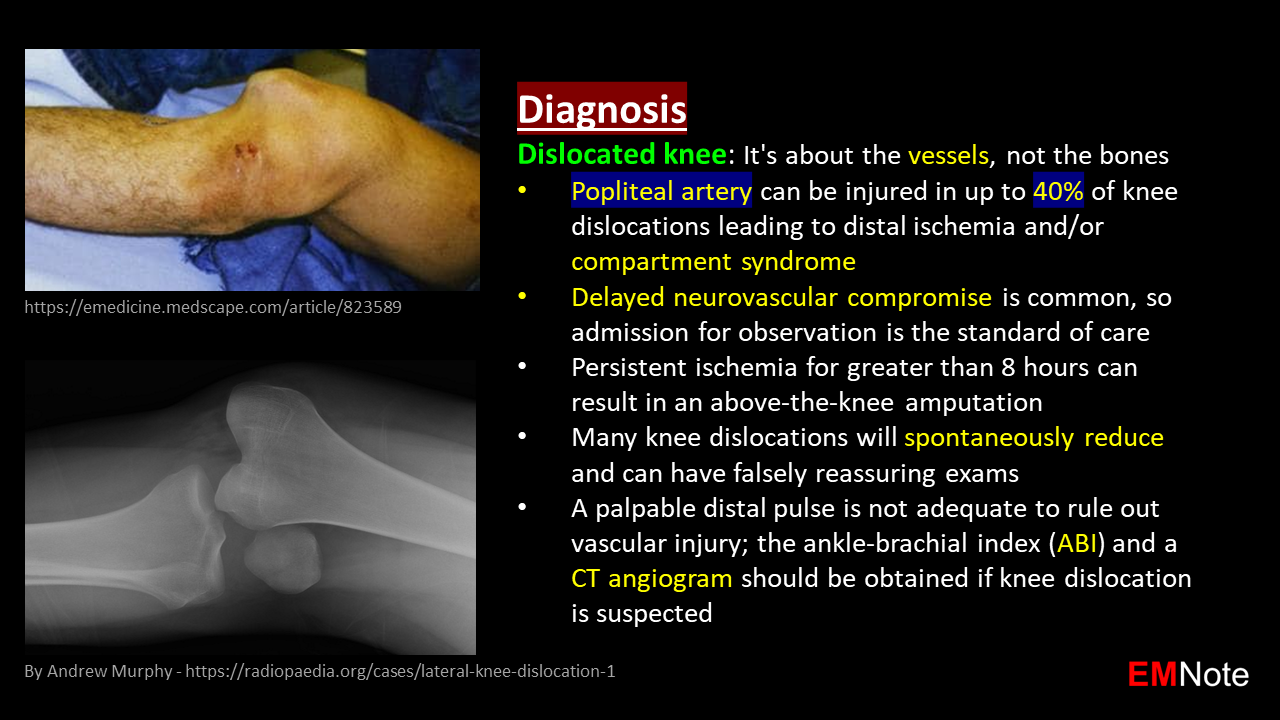 Visual Diagnosis Part 8
Ludwig's angina Ludwig's angina is a rapidly progressive bacterial infection of the submandibular, sublingual, and submental spaces beneath the tongue, resulting in severe cellulitis of the neck and floor of the mouth. Early recognition is critical due to the high risk of airway obstruction. Symptoms of Ludwig's angina include tongue elevation, dysphagia, drooling, trismus (jaw locking), and muffled speech. Immediate hospitalization and aggressive antibiotic therapy with airway management are essential to prevent life-threatening complications. The main pathogens are Streptococcus viridans, Staphylococcus aureus, and anaerobes. Rectus sheath hematoma Rectus sheath hematoma is a collection of blood within the rectus abdominis muscle sheath. Rectus sheath hematoma can arise from diverse causes, including traumatic injury, spontaneous tears in blood vessels, or complications of anticoagulation therapy. Rectus sheath hematoma is often unilateral and exacerbated by straining or coughing. Management of Rectus sheath hematoma range from observation for small cases to surgical intervention for larger or actively bleeding hematomas. Pulmonary and right atrial thrombus Risk factors of pulmonary embolism include: recent surgery, prolonged immobilization, and deep vein thrombosis (DVT). The diagnostic test of choice for pulmonary embolism is CT pulmonary angiography. Prompt treatment with anticoagulants is crucial to prevent further complications. Slipped capital femoral epiphysis (SCFE) Salter-Harris fracture type I. The risk factors of slipped capital femoral epiphysis include: obesity, teenager, male, and Legg-Calvé-Perthes disease. Slipped capital femoral epiphysis can occur bilaterally in 20-40% of cases. Severe slips (greater than 50 degrees) need urgent surgery within 6 to 12 hours to prevent further damage and complications. Chvostek's sign and Trousseau's sign Chvostek's sign is a clinical finding associated with hypocalcemia, elicited by tapping the facial nerve in front of the ear, just below the cheekbone. A positive Chvostek's sign is indicated by a twitch of the facial muscles on the same side of the face as the tap. Trousseau's sign is another clinical finding associated with hypocalcemia, elicited by inflating a blood pressure cuff above systolic pressure on the arm, a positive test is confirmed if the hand involuntarily contorts into a "main d'accoucheur" pose (wrist bent, thumb drawn in, fingers arched). Additional symptoms of hypocalcemia include tingling in the lips, tongue, fingers, and feet, muscle aches, laryngospasm, tetany, seizures, and arrhythmias. Knee dislocation Keep in mind that, knee dislocation is about the vessels, not the bones. Popliteal artery can be injured in up to 40% of knee dislocations leading to distal ischemia and/or compartment syndrome. Delayed neurovascular compromise is common, so admission for observation is the standard of care. Persistent ischemia for greater than 8 hours can result in an above-the-knee amputation. Many knee dislocations will spontaneously reduce and can have falsely reassuring exams. A palpable distal pulse is not adequate to rule out vascular injury; the ankle-brachial index (ABI) and a CT angiogram should be obtained if knee dislocation is suspected. Omental cake Omental cake refers to CT images showing abnormally thickened "greater omentum" due to infiltration by other types of soft-tissue, ascites, or chronic inflammation resulting in a cake-like appearance. The most common etiology of omental cake is ovarian cancer. Other causes include gastric cancer, colon cancer, pancreatitis, peritonitis, Crohn's disease, ascites, and tuberculosis. |

Author
|