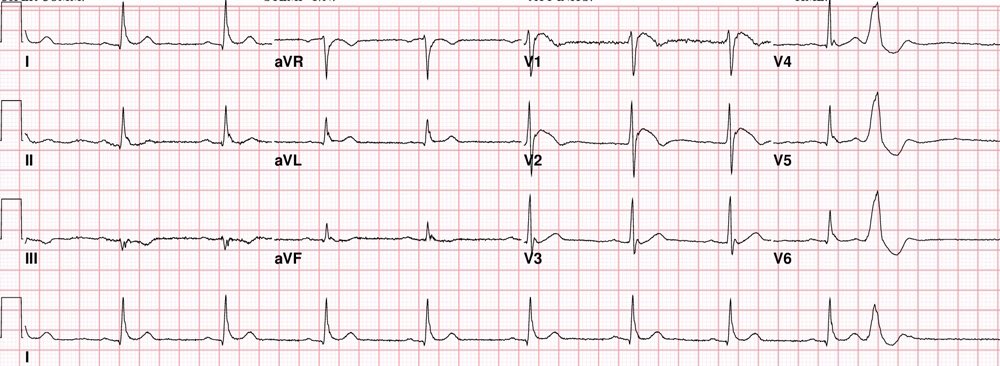
   https://twitter.com/EM_RESUS/status/852579079069065218 Brugada Syndrome: This is an ECG abnormality with a high incidence of sudden death in patients with structurally normal hearts. Brugada syndrome is due to a mutation in the cardiac sodium channel gene. This is often referred to as a sodium channelopathy. Familial clustering and autosomal dominant inheritance has been demonstrated. ECG changes can be transient with Brugada syndrome and can also be unmasked or augmented by multiple factors, such as fever, ischemia, drugs, hypokalemia, etc. ECG diagnosis: Type 1 (Coved ST segment elevation >2mm in >1 of V1-V3 followed by a negative T wave) is the only ECG abnormality that is potentially diagnostic. This has been referred to as Brugada sign. The other two types of Brugada are non-diagnostic but possibly warrant further investigation. Type 2 has >2mm of saddleback shaped ST elevation. Brugada type 3 can be the morphology of either type 1 or type 2, but with <2mm of ST segment elevation. Clinical Management: Syncope and cardiac arrest are common clinical manifestations. In many cases, cardiac arrest occurs during sleep or rest. To date, the only treatment that has proven effective in treating ventricular tachycardia and fibrillation and preventing sudden death in patients with Brugada syndrome is implantation of an automatic implantable cardiac defibrillator (ICD). No pharmacologic therapy has been proven to reduce the occurrence of ventricular arrhythmias or sudden death; however, theoretically, drugs that counteract the ionic current imbalance in Brugada syndrome could be used to treat it, for example, quinidine. http://lifeinthefastlane.com/ http://circep.ahajournals.org/content/5/3/606  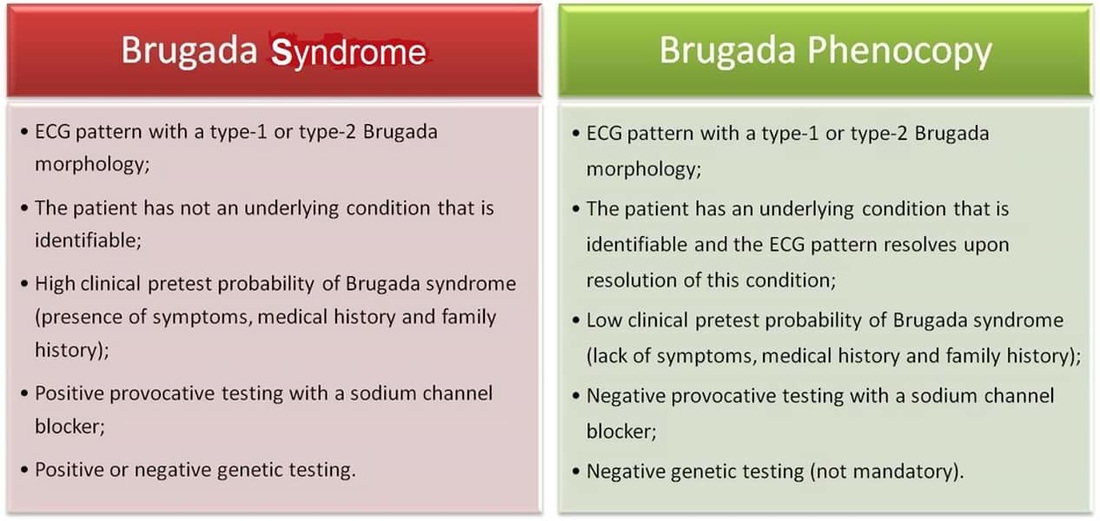 Please take note that Brugada ECG pattern may not be true Brugada syndrome, but merely Brugada phenocopy. Reference: Brugada syndrome and Brugada phenocopy. The importance of a differential diagnosis ~ International Journal of Cardiology 210 (2016) 25–27 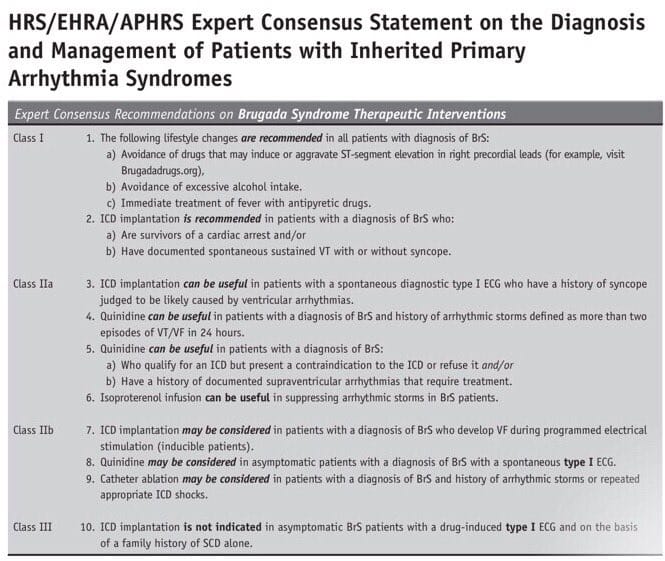
1 Comment
|

Author
|